Adhd students and the curriculum in Australia
Providing appropriate support for students with ADHD is integral to their development as a socially and emotionally integrated young adult.
ADHD is a clinically diagnosed learning disorder, and as the most highly researched behaviour disorder, there is a multitude of resources available about treatment, diagnosis and management strategies. Overwhelming evidence shows that ADHD is primarily an inherited disorder, meaning that the presence of cognitive deficiencies are not linked to diet, parenting or computers, although, in the same way as these factors can affect all children negatively, the problematic behavioural symptoms of the ADHD child can become magnified.
Research overwhemingly supports the use of stimulant medications for this disorder.
Students with ADHD possess deficiencies in attention and self management - which are essential cognitive functions in developing independence and self-regulation. Therefore, the ADHD student in a school context needs to be supported by assisting the student in performing executive functions. If ADHD students are not diagnosed, treated and supported effectively throughout their childhood and adolescence, it can lead to serious impairments in learning, social relationships, family life and adult occupations, and is linked to a significant increase in school dropout, under performance at work and substance misuse.
ADHD is a clinically diagnosed learning disorder, and as the most highly researched behaviour disorder, there is a multitude of resources available about treatment, diagnosis and management strategies. Overwhelming evidence shows that ADHD is primarily an inherited disorder, meaning that the presence of cognitive deficiencies are not linked to diet, parenting or computers, although, in the same way as these factors can affect all children negatively, the problematic behavioural symptoms of the ADHD child can become magnified.
Research overwhemingly supports the use of stimulant medications for this disorder.
Students with ADHD possess deficiencies in attention and self management - which are essential cognitive functions in developing independence and self-regulation. Therefore, the ADHD student in a school context needs to be supported by assisting the student in performing executive functions. If ADHD students are not diagnosed, treated and supported effectively throughout their childhood and adolescence, it can lead to serious impairments in learning, social relationships, family life and adult occupations, and is linked to a significant increase in school dropout, under performance at work and substance misuse.
Characteristics and identification
A student with ADHD, like any student, has different abilities and behaviours. However, the presence of ADHD in a child will be manifested by particular characteristics which are caused by the way the ADHD brain controls thinking, learning and behaviour. (Larkin, 2012 p. 20)
These characteristics or symptoms are:
There are certain criteria that needs to be met for these characteristics to be identified as symptoms of ADHD, which are clinically assessed by a pediatrician, child psychiatrist or child psychologist. For a diagnosis of ADHD, at least six criterion for each characteristic must be present in the child for at least six months, to a level that is problematic for the student's social and academic functioning and to a degree that is inconsistent with the normal developmental level. (Vic Health Channel, Attention Deficit Hyperactivity Disorder - diagnosis)
Only specialist clinical professionals (pediatrician, child psychiatrist or child psychologist) can diagnose ADHD and prescribe medication to address the neurological imbalances in the brain's functioning.
These characteristics or symptoms are:
- Difficulty paying attention (difficulty in/lack of concentration, easily distracted from tasks, failing to complete homework or follow through, forgetful)
- Impulsivity (often interrupts or answers before questions are completed, often interrupts conversations, has problems waiting in line)
- Overactivity (often figets or squirms, has difficultly playing quietly, talks excessively, runs or climbs excessively in situations where it is inappropriate, finds it hard to remain seated when required, 'on the go')
There are certain criteria that needs to be met for these characteristics to be identified as symptoms of ADHD, which are clinically assessed by a pediatrician, child psychiatrist or child psychologist. For a diagnosis of ADHD, at least six criterion for each characteristic must be present in the child for at least six months, to a level that is problematic for the student's social and academic functioning and to a degree that is inconsistent with the normal developmental level. (Vic Health Channel, Attention Deficit Hyperactivity Disorder - diagnosis)
Only specialist clinical professionals (pediatrician, child psychiatrist or child psychologist) can diagnose ADHD and prescribe medication to address the neurological imbalances in the brain's functioning.
Implications for classroom teachers
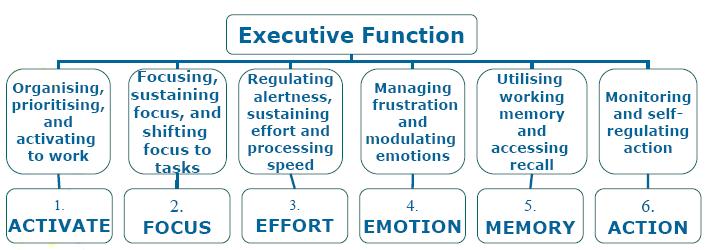
As students with ADHD have problems with essential executive functioning (see diagram below), teachers need to support students through accommodation - implementing tasks which do not require executive functions, and supporting their activation functions in breaking down instructions and reminding.
Other possible learning and behavioural difficulties may co-exisit with ADHD such as literacy, speech and language difficulties, developmental disorders, global learning difficulties, ASD and social disorders. With the possibility of a combination of learning and/or behavioural disorders implies that teachers and counselors should be aware of marked characteristics which indicate particular difficulties, and if any are identified, to address with appropriate learning support and referral to medical/psychological specialists.
Early identification, diagnosis and appropriate long-term support is essential for the student to effectively access the curriculum.
Left untreated and unsupported, subsequent negative emotional and behavioural development can occur:
Age 6 - low self-esteem, minor learning and social difficulties
Age 10 - disruptive behaviours, poor social skills, learning delay
Age 14 - challenging behaviour, ODD
(Larkin, p. 25)
Other possible learning and behavioural difficulties may co-exisit with ADHD such as literacy, speech and language difficulties, developmental disorders, global learning difficulties, ASD and social disorders. With the possibility of a combination of learning and/or behavioural disorders implies that teachers and counselors should be aware of marked characteristics which indicate particular difficulties, and if any are identified, to address with appropriate learning support and referral to medical/psychological specialists.
Early identification, diagnosis and appropriate long-term support is essential for the student to effectively access the curriculum.
Left untreated and unsupported, subsequent negative emotional and behavioural development can occur:
Age 6 - low self-esteem, minor learning and social difficulties
Age 10 - disruptive behaviours, poor social skills, learning delay
Age 14 - challenging behaviour, ODD
(Larkin, p. 25)
Brown, TE. Manual for Attention Deficit Disorder Scales for Children and Adolescents; 2001
SCHOOL AND COMMUNITY support for students with ADHD
The responsibility for supporting students with ADHD has largely remained with special education practitioners or classroom teachers. Classroom teachers, therefore, need to modify and scaffold tasks, provide direct instruction, find suitable physical classroom arrangements and work closely with school leadership, school counselors or psychologists and parents in devising appropriate Individual Learning Plans. These learning plans may involve behavioural and academic goals or programs, according to the needs of the student.
In the wider community, there is a myriad of clinical and counselling support available for students with AD/HD. It is important that students get the appropriate medical and psychological support which must be found outside the school. Students with AD/HD need to meet regularly. Some of these organisations are listed below.
The ADHD Coalition of Victoria Inc. http://www.adhdcoalitionvic.org.au/
http://www.psychology.org.au/community/adhd/
Hyperactive Children’s Association of Victoria (ACTIVE) Ph: 9650 2570 (The Better Health Channel, www.betterhealth.vic.gov.au)
In the wider community, there is a myriad of clinical and counselling support available for students with AD/HD. It is important that students get the appropriate medical and psychological support which must be found outside the school. Students with AD/HD need to meet regularly. Some of these organisations are listed below.
The ADHD Coalition of Victoria Inc. http://www.adhdcoalitionvic.org.au/
http://www.psychology.org.au/community/adhd/
Hyperactive Children’s Association of Victoria (ACTIVE) Ph: 9650 2570 (The Better Health Channel, www.betterhealth.vic.gov.au)
government POLICIES AND LEGISLATION
"There are no Australian ADHD-specific federal or state policies. Neither is it considered a specific learning disability (NH&MRC, 1997). Whereas the Commonwealth Disability Discrimination Act (DDA) covers categories in the Diagnostic and Statistical Manual of Mental Disorders (APA, 2000) (thus indirectly defining ADHD as a disability), most states use their own equal opportunity legislation (which does not include ADHD as a disability) as the basis of special education policy.” (Prosser et. al., 2002)
FURTHER INFORMATION AND SUPPORT RESOURCES
Teaching strategies
http://www.mindspace.bravepages.com/strategies.htm
_________________
REFERENCES
Larkin, G. (2012). Risk Factors for Students Accessing the Curriculum 2. EDFD547: Diversity in the Classroom. Melbourne: Australian Catholic University.
Prosser, B., Reid, R., Shute, R., Atkinson, I. (2002) ‘Attention deficit hyperactivity disorder: special education policy and practice in Australia’ From Australian Journal of Education. 46.
http://www.mindspace.bravepages.com/strategies.htm
_________________
REFERENCES
Larkin, G. (2012). Risk Factors for Students Accessing the Curriculum 2. EDFD547: Diversity in the Classroom. Melbourne: Australian Catholic University.
Prosser, B., Reid, R., Shute, R., Atkinson, I. (2002) ‘Attention deficit hyperactivity disorder: special education policy and practice in Australia’ From Australian Journal of Education. 46.
